Chapter 1
Restrictions during the pandemic must be as proportionate as possible. There is no need to impose full restrictions on people who we know are at a greatly reduced risk of transmitting Covid-19.
Vaccines significantly reduce the risk of death, hospitalisation and transmission. Once vaccines are available to all adults in the UK, and for as long as restrictions are deemed necessary at all, any venue or setting choosing to become vaccine only should be free to remove most restrictions enabled through a robust Covid Pass that allows individuals to prove their vaccine and/or testing status.
The same principle should apply to travel. A sensible approach would be to take account of an individual’s vaccine status when it comes to testing and quarantine requirements, while reducing the prohibitive costs of tests.
Chapter 2
During the pandemic to date, restrictions intended to reduce the spread of disease have necessarily treated populations as largely homogenous groups for which there is no distinction between individuals when it comes to their risk of being infected by, or transmitting, Covid-19. This means that tools to contain the virus have been necessary but blunt: we’ve seen national lockdowns, regional-tier systems and entire schools shut down following suspected outbreaks.
Vaccinations have changed this. Their effectiveness at reducing transmission, now proven beyond any doubt, means that different people carry different risks when it comes to spreading the virus. Ultimately, the fully vaccinated are much less likely to infect others – approximately up to 50 per cent less likely.[_] Furthermore, they are less likely to die, be hospitalised or develop Covid-19 symptoms compared to pre-vaccine.
Simply put, vaccine status matters.
It is therefore critical that individuals are able to prove their vaccine status. In this paper, we set out the digital health pass infrastructure that will need to be introduced to enable an individual to prove their vaccine status. This goes beyond the current NHS App: a globally interoperable system of health passes is required to allow citizens to prove their status in a secure, privacy-preserving way. The health pass needs to be usable both by national border authorities and other organisations within countries. It should also include the ability to demonstrate time-restricted testing status for those who aren’t able to be vaccinated.
With this ability to securely prove vaccination status, we can move beyond blunt, catch-all tools and align with other countries by removing certain restrictions for the fully vaccinated – thereby enabling us to sustainably reopen the economy. We offer recommendations across two areas: travel and in domestic settings.
For travel, we propose that anyone who is fully vaccinated should be free to travel to and from any country currently designated as green without any quarantine period or testing required. Of course, the greatest risk with reopening borders in this way is that we expose ourselves to new variants – a real threat exemplified by the Delta variant at present. That’s why anyone arriving in the country – vaccinated or unvaccinated – from an amber country should be subject to an NHS PCR test at low cost, with any positives sent for genomic sequencing. This will ensure they don’t have a new variant resistant to antibodies that could undo all the hard work to date. We propose using latent NHS PCR capacity and incorporating lateral flow tests, sufficient to detect infectiousness, into the pre- and post-travel testing regime. These tests should be easily available – and our proposals set out how we can harness existing resources to deliver this.
Domestically, we propose that any venue or setting that wants to admit only those who have been vaccinated should be permitted to do so – and this should be enabled through the aforementioned Covid Pass. Venues adopting a vaccine-only policy – be it a cruise liner, a sporting stadium or a restaurant – would then be subject to fewer restrictions. A government enabled Covid Pass would mean that citizens only need one app, rather than a confusing myriad of different passes for different places. This enabling role of government is important: no venue should have to become vaccine only and every setting should have the option of remaining open to the unvaccinated as well as the vaccinated – accounting for any increase in risk with increased restrictions.
The ultimate objective should be to have no Covid passes and no restrictions whatsoever. Where and when this is possible, it should be adopted without delay. It may even be that a Covid Pass is turned on and off as new variants that threaten particular types of vaccines are identified, or as we learn more about how long immunity lasts as well as the need for booster shots. However we choose to move forward, for as long as the world goes largely unvaccinated and the risk of a new variant remains significant, it’s vital that we have an alternative to the blunt tool of lockdowns to enable the country to live freely and safely.
Chapter 3
Vaccination significantly reduces the risk of hospitalisation and death from Covid-19. In addition to last year’s promising clinical trial results, real-world data from vaccine rollouts around the world has validated those early results. In the UK, researchers from the Universities of Edinburgh, Strathclyde, Aberdeen, Glasgow and St Andrews and Public Health Scotland (PHS) analysed a data set covering the entire Scottish population of 5.4 million people. The study found that the Pfizer-BioNTech and Oxford-AstraZeneca vaccines were shown to reduce the risk of hospitalisation from Covid-19 in up to 85 per cent and 94 per cent of cases respectively.[_]
Pre-print data from Public Health England (PHE) shows that individuals who receive a single dose of the AstraZeneca vaccine have an approximately 80 per cent lower risk of death from a Covid-19 infection compared to unvaccinated individuals. The report also found that the Pfizer jab reduces the chances of dying from Covid-19 by approximately 80 per cent after one dose, a figure that rises to 97 per cent after two doses.[_]
Because of the incredibly efficient rollout taking place in Israel and the extensive data being collected there, Israel has been able to provide early insights into the benefits of vaccinations against Covid-19. Data from one study published in the Lancet in May highlights the effectiveness of vaccines in Israel (in this case, Pfizer only) in preventing hospitalisation and death:[_]
During the study period, of the 154,648 people infected by Covid-19, aged 16 years and over, 71 per cent (109,876) were unvaccinated and 4.1 per cent (6,266) were fully vaccinated.[_]
Of the 54,677 people aged 16 years and over who had symptomatic infections, 71.4 per cent (39,065) were unvaccinated and 3.1 per cent (1,692) were fully vaccinated.
Of the 7,694 people aged 16 years and over who were hospitalised with Covid-19, 71.8 per cent (5,526) were unvaccinated and 7.7 per cent (596) were fully vaccinated.
Of the 4,481 people aged 16 years and over with Covid-19-related severe or critical hospitalisations, 71.4 per cent (3,201) were unvaccinated and 8.1 per cent (364) were fully vaccinated.
Of the 1,113 people aged 16 years and over who died from Covid-19, 64.2 per cent (715) were unvaccinated and 12.4 per cent (138) were fully vaccinated.
It is also becoming increasingly clear that vaccinated individuals are less likely to catch and transmit the virus. In April, PHE published the results of a large-scale study of Covid-19 transmission involving more than 365,000 households that consisted of both vaccinated and unvaccinated individuals.
The data found that being vaccinated with either Pfizer or AstraZeneca (the only two vaccines in widespread use in the UK at the time), reduced the likelihood of onward virus transmission by 40 to 60 per cent. This means that if someone became infected after being vaccinated, they were only around half as likely to pass their infection on to others compared to infected unvaccinated individuals.[_]
Data from Israel sheds light on why this may be the case. One study analysed nose swabs from nearly 5,000 vaccinated individuals who were infected with Covid-19 and compared those with nose swabs from infected individuals who had not been vaccinated. Researchers found significantly lower amounts of the virus in the swabs from vaccinated individuals compared to the swabs from the unvaccinated. It is likely that the smaller viral loads found in vaccinated individuals contributes to the reduced transmissibility of the virus because higher viral load in the nose has been linked to greater infectiousness and increased risks of onward transmission.[_]
To date, over 39 million people in the UK have had a first dose of a vaccine, which is almost 75 per cent of the adult population. More than 26 million people have had a second dose, with this figure rapidly increasing as the UK is averaging more than 400,000 second doses per day.[_]
The government’s current target is to have offered a first dose to all adults by the end of July 2021. It has yet to be announced when the vaccine will be approved for children aged 12 and older or when we can expect the jab to be extended to this youngest age group.
However, offering a jab to everyone is just part of the task because uptake among the population is a more accurate measure of how much protection we can expect from vaccines. According to data collected up until 31 May, the estimated vaccine uptake in the UK is around 74.9 per cent for first doses and 48.9 per cent for second doses.[_]
Estimated vaccine take-up as of 31 May by age group for London – one dose
Estimated vaccine take-up as of 31 May by age group for London – two doses
According to data collected up until 23 May, vaccine uptake by age group in England among NHS-registered individuals is as follows:
Estimated vaccine take-up as of 23 May by age group in England – one dose
Source: ONS (Estimates were made based on the number of vaccines administered to English residents with NHS numbers and the percentages were calculated using these figures and the 2019 mid-year population estimates, which are the most recent official statistics on population size and the best publicly available population estimates).Source: ONS (Estimates were made based on the number of vaccines administered to English residents with NHS numbers and the percentages were calculated using these figures and the 2019 mid-year population estimates, which are the most recent official statistics on population size and the best publicly available population estimates).[_]
Estimated vaccine take-up as of 23 May by age group in England – fully vaccinated
Source: ONS (Estimates were made based on the number of vaccines administered to English residents with NHS numbers and the percentages were calculated using these figures and the 2019 mid-year population estimates, which are the most recent official statistics on population size and the best publicly available population estimates).[_]
Although these figures are estimates for uptake among each age group in London and then in England, additional ONS data supports the assumption that figures for the whole of the UK are likely to be similar. In terms of attitudes towards vaccination, the data below shows that the take-up rates above could continue to grow, even for the older age groups that have long been able to book a jab. For example, 95 per cent of adults in the UK have either already received a jab or would be likely to accept a Covid-19 vaccine if offered. The breakdown by age groups roughly mirrors the trends shown above in figures 1–4:[_]
99 per cent of individuals aged 70 and older have either received a jab or responded that they were likely to accept a jab when offered.
98 per cent of individuals aged 50–69 have either received a jab or responded that they were likely to accept a jab when offered.
94 per cent of individuals aged 30–49 have either received a jab or responded that they were likely to accept a jab when offered.
85 per cent of individuals aged 16–29 have either received a jab or responded that they were likely to accept a jab when offered.
Our objective remains to get as many people vaccinated as quickly as possible.
Chapter 4
The fact that there is no distinction between those who are fully vaccinated and those who are not has also led to a lowest-common-denominator approach to applying restrictions within the UK. Under current Covid-19 guidance issued by the Cabinet Office, those who have received the vaccine should continue to take recommended precautions to avoid infection, even though their chances of doing so are much lower.
This naturally has a significant impact on individual freedoms, the ability of businesses to operate and, in turn, on the economy. Current Covid-19 guidance in England indicates that most businesses (for example, indoor entertainment and attractions, as well as indoor and outdoor events such as live performances, sporting events and business events) can reopen. But Covid-secure guidance will remain in place and businesses may not cater for groups larger than the legal limits. In general, Covid-secure rules include social distancing, the requirement to wear a face covering indoors (including on public transport) and reduced capacity in certain settings (for example, indoor venues and attractions must only be accessed in groups of up to six people or larger groups consisting of no more than two households, unless an exemption applies). All legal limits on social contact are expected to be lifted from 21 June. However, this is subject to the criteria ensuring Covid-19 infection rates do not overwhelm the NHS, and there is a strong possibility this date may need to be delayed. There is also a risk that restrictions may be reimposed when necessary (such as when there are new variants of concern). That being the case, it makes sense to target the restrictions as accurately as possible, to minimise cost and inconvenience, while still controlling the spread of the virus.
The economic and social cost of domestic restrictions is substantial. Sectors involving more face-to-face contact, including hospitality and entertainment, have been particularly hard hit. According to Office for National Statistics (ONS) data, output in the arts and entertainment sector fell sharply in January 2021 and was 35 per cent below its February 2020 (pre-pandemic) level, while the accommodation and food sector was 59 per cent below. The wholesale and retail, and transportation, sectors also saw large falls in output in January 2021[_]. Due to current Covid-measures, venues such as museums and galleries are now operating at about 20 per cent of their pre-pandemic attendance, and many cultural organisations will struggle to survive[_]. This dramatic reduction in activity will inevitably impact employment, wellbeing and the economic and cultural fabric of our society.
To minimise the damage, we should allow most[_] businesses and other organisations the flexibility to remove certain restrictions for those who are at a reduced risk of transmitting Covid-19 – that is, anyone who is fully vaccinated, or who has taken and received a recent negative lateral flow test. This would pave the road to recovery and allow for fuller participation in the country’s social, economic and cultural offers. It would also provide an invaluable tool to manage the spread of new variants, without resorting to a full lockdown or blanket restrictions.
The approach of restricting entry to public spaces based on health status has been shown to be effective at reducing transmission. At a number of pilot events held in Liverpool recently, ticket holders were required to show results of negative lateral flow tests, upon which they could gain entry without the need for face masks and social distancing. More than 13,000 people were reported to have attended two nightclub events, a music festival and a business conference in April and May, and only 11 people later tested positive for Covid-19.
To implement this conditional relaxation of restrictions for those at reduced risk, an effective digital-health pass solution will be needed. A number of countries have now put health passes in place. Israel’s Green Pass (now withdrawn due to low case rates) provided a simple and straightforward way for citizens to access and share live health data in order to enter venues such as gyms, restaurants, theatres and cinemas, sporting venues, hotels and cultural events.[_] A similar Covid certificate has been rolled out in Denmark since April. The Coronapas certifies that someone has either been fully vaccinated, has tested negative in the previous 72 hours, or has tested positive two to 12 weeks earlier, thereby conferring them with immunity to the virus. The pass will not be used for travel right away but it grants access to hairdressers, restaurants, cinemas, tattoo parlours and driving schools.
The UK government is currently reviewing the case for introducing health passes (known as Covid certificates) but it has announced that it will not mandate their use for entry to mass events. We recommend that businesses be given the choice to relax social-distancing rules for those who can demonstrate they are at reduced risk of transmitting the virus. However, government will need to play the role of facilitator whether or not it decides to allow conditional relaxation of restrictions. On this point, several large firms have already announced that they will require their employees and/or their customers to be vaccinated. To make this work efficiently, a digital health pass will be needed. Given that one is required to facilitate travel, the additional cost to implement the same system within the UK should be marginal.
Recommendation
As soon as vaccines are available to all age groups, a wide range of organisations should have the option to restrict entry to their premises to those who have either been fully vaccinated or have had a recent negative lateral flow test. If they take up this option, they should be allowed to operate with no restrictions on capacity, no observed social distancing and without requirements to wear a face covering. This would allow a wide range of settings – shops, bars and restaurants, gyms, sports and cultural venues, offices and factories – to return to operating as normal.
We set out further recommendations on the design and functionality of the health pass app later in this paper.
Chapter 5
We believe that those who are fully vaccinated should be given additional freedoms when travelling internationally.
Based on the evidence above, it is clear that a traveller who has been fully vaccinated poses a lower risk compared to someone unvaccinated. To ensure our travel system works correctly, this should be properly reflected in policy as soon as possible.
As more and more of the population are vaccinated with two doses, the more travel policy needs to reflect this. This change in policy would be undertaken in a step-by-step way, with a short- and then medium-term strategy.
The existing travel system is confusing and costly, taking no account of someone’s vaccine status
In the absence of a government lead, the private sector is taking steps to refine the travel system by taking into account an individual’s vaccine status.
For instance, in January, Saga Cruises announced that it would require all passengers to be fully vaccinated in order to join a cruise. Saga delayed restarting its travel packages until May to give customers and employees enough time to get jabs.
Travel Tests Are Prohibitively Expensive
Not only does the existing and confusing system fail to take vaccine status into account, it is also prohibitively expensive and complex. Recent research by the Travel Association (ABTA) and the Airport Operators Association found that the cost of PCR testing for international travel from the UK is twice as expensive as testing in other European countries. A UK pre-departure PCR test costs on average £128 ($180) per person, while the average pre-departure test cost across eight key destinations comes to just under £62 ($87).[_]
In terms of the tests required upon returning to the UK, the prices are even more disproportionate to the cost of travelling. Prices for PCR kits for returning travellers range from £150 ($211) to £350 ($493) per testing kit.[_] Given that each person travelling will need their own kit, this will add a significant cost to family holidays. Even travellers to countries on the green list will need a kit, albeit just for day two of their return, whereas those travelling to countries on the amber and red lists will need a PCR test for both day two and day eight.
An individual travelling from the UK to a European destination will pay an average of £306 for testing because they will need a UK pre-departure test; another pre-departure test in their destination country at the end of their holiday; and a post-arrival test in the UK if they have flown from a green list country, or two post-arrival tests if returning from an amber or red list country.[_]
This is on top of any related costs incurred by needing to isolate at home or a hotel if travelling from a red list country, which currently stands at £1,750 ($2,468) for an adult and £325 ($458) per child aged between 5 and 11.[_]
Travel expert Virginia Messina recently commented, calling the system “unworkable”. She went on to say: “It’s not just booking the test, it’s the expense of it, if you think of a family of four it really changes the economics of travel. If you travel to a country … which is still requiring PCR, one test can be up to £200 ($282), then you need to take three more when you arrive back in the UK; the economics don’t work out.”[_]
A poll conducted by the insurer Battleface found that this sentiment was shared by a vast majority of respondents. Of the 2,000 people surveyed, just four per cent would be prepared to pay £75 ($105) or more for a PCR test to travel internationally and one third of people weren’t prepared to pay anything for testing before travelling. The survey reported that respondents were willing to pay an average cost of £22 ($31) per person for a PCR test.[_]
Figure 6 – The international situation, as shown by travel requirements for fully vaccinated individuals by country
Case Study
Case study: Gibraltar – The Lateral Flow Versus PCR Test
Gibraltar has replaced PCR tests with lateral flow tests upon arrival for fully vaccinated individuals as well as unvaccinated individuals arriving from countries on the green list. Fully vaccinated travellers do not need to quarantine and will only be subject to a PCR test if they are arriving from a red list country. The arrivals process for fully vaccinated individuals entering Gibraltar looks like this:
Test upon arrival: As a result of growing concerns around the Delta variant, Gibraltar now uses lateral flow tests free of charge for all travellers flying into the country, which are conducted at the airport immediately following arrival; PCR tests conducted at the airport immediately following arrival if travellers has been to a red list country in the last 14 days.
Quarantine: No self-isolation required.
Further tests while in Gibraltar: None if travelling from a green list country. A follow-up lateral flow test or PCR test will be administered on day 5 of the visit if the individual came from an amber or red list country respectively.
The European Union has announced proposals that from 1 July, it will lift all obligations on those who are fully vaccinated. The system will allow EU member states to issue a digital Covid passport so that citizens can show their vaccination status and travel freely.
The same will apply to someone who has had a negative Covid test or who can show they have recovered from infection. The European Commission has set out a standard validity period of 72 hours pre-travel for PCR tests and 48 hours for lateral flow tests.
Principles of a New Strategy
Based on both the state of play within the UK and emerging best practice internationally, we propose a recalibration of our travel strategy. This change in strategy is geared towards meeting the following aims:
Reducing cost.
Removing bureaucracy.
Simplifying to remove confusion.
Basing policy on individual, not collective, risk.
Fixing the current travel system will require taking better account of the risk each passenger poses and removing friction within the process. As travel continues to open in the coming months and years, a simple and robust system is required. Given the starting point – a confusing UK system and absent global architecture – it will take time and a series of carefully calibrated steps to reach the right position on travel. Short term, we think this will involve making use of NHS PCR-testing infrastructure, and then longer term moving to fully embrace the possibilities of lateral flow testing. The immediate priorities should be to reduce cost from the system and better reflect the differing Covid statuses of travellers.
This can be achieved in the following ways:
Reduce the Cost of Testing. At the moment pre- and post-travel testing is being done with PCR tests, provided by private testing companies. The costs of these tests can vary (on average, £128/$180) but prices differ greatly.
To reduce the costs from the testing regime, we propose utilising NHS PCR-testing capability to conduct travel testing for amber countries. This should come at a nominal charge to travellers compared to current prices.
At present, NHS PCR capacity is around 650,000 tests, with only about a third being regularly used. This provides significant headroom for NHS PCR tests to be used for travel testing passengers arriving from amber countries. Daily passenger numbers arriving in the UK are in flux. For April 2021, around 15,000 air passengers were arriving per day. For September last year, a high point in the past 12 months, it was around 100,000 per day. This could easily be accommodated via the NHS system. Where a shortfall arises in capacity for PCR testing, the travel sector should fund additional testing capability with minimal costs for passengers.[_]
PCR testing capacity in the UK, May 2020 – May 2021
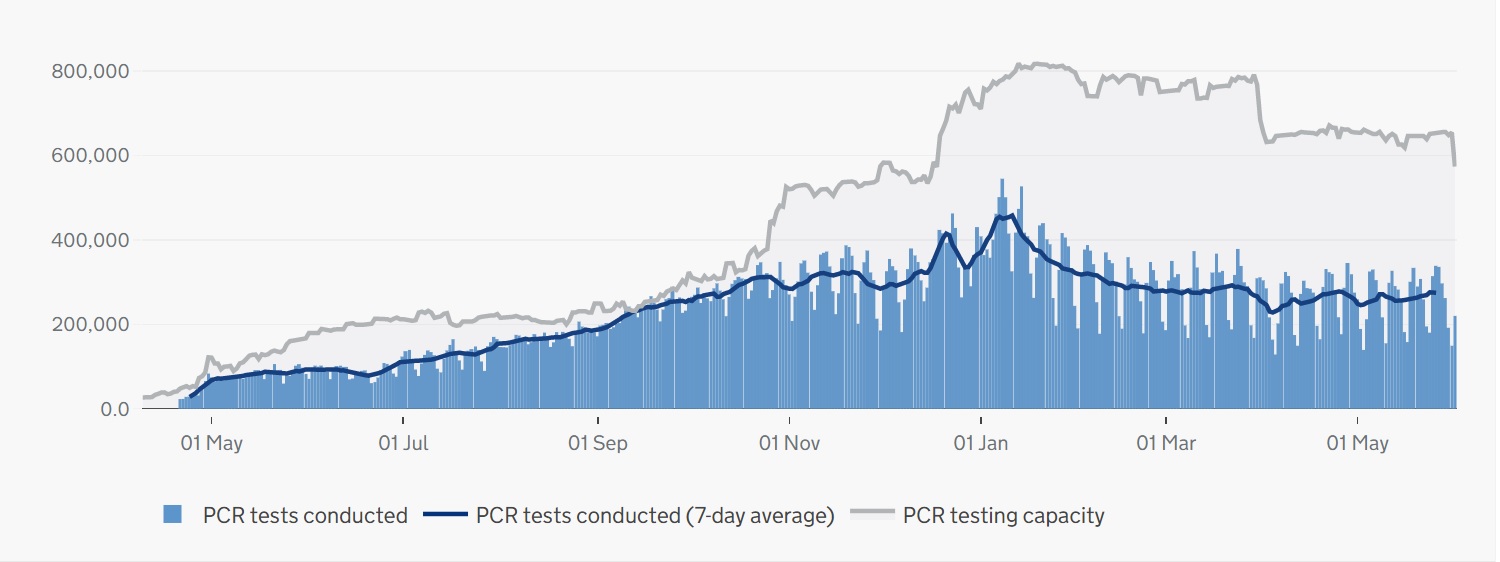
Source: https://coronavirus.data.gov.uk/
Testing costs for red list countries would remain the same and be accessed through the existing system.
NHS Testing to Travel: Disrupting (But Not Decimating) the Market
As it stands, tests to travel are extortionately priced and particularly punitive for families. For example, a family of two adults with two children could expect to pay thousands for their testing requirements. While it’s important that we have a flourishing ecosystem of private testing providers to keep capacity high and offer fast-turnaround solutions, it is clear costs need to come down. Therefore, the NHS – with around 60 per cent of its PCR testing capacity available – should enter the market and offer PCR tests for travel at a low cost, particularly orientating these towards families.
This will bring other providers’ prices down and ensure the testing market becomes more family friendly. Longer term, we propose that free, sufficiently effective lateral flow tests replace PCR tests for travel testing requirements.
The role of vaccine status – a theme running through this paper – will also ensure that travel costs become less prohibitive by removing the need for testing altogether in certain scenarios.
Focus on Individual, Not Collective, Risk. The UK should move to a position where it differentiates between those who are vaccinated and those who are unvaccinated.
Figure 8 – Moving to a system in which the UK differentiates between the vaccinated and unvaccinated
Some Reds Are So Light, They’re Amber
The red list plays a vital role in reducing the introduction of dangerous variants into the UK. It should essentially serve as a “Do Not Travel Here” list, which is why it is important that serious thought is given to the countries included on it. Countries whose Covid-19 situation is concerning, whether this is because of high case numbers or the dominance of a variant of concern, need to remain on the red list. However, not all countries on the current red list pose the same level of risk.
The current red list includes countries with vastly different situations. India, for instance, has had more than 100,000 cases per day for the past two months. In Rwanda, by contrast, daily new cases are now regularly well below 100. Similarly, over the past two weeks Zimbabwe has averaged 26.6 cases per one million people while Turkey, over the same period, averaged 1,224.5 cases per million. This stark contrast should require the country categories (i.e. green, amber and red) to allow further differentiation within them. Although there are other factors to be considered, such as the level of testing and vaccination rates, it is clear that not all red list countries pose the same level of risk to travellers. Using the above example, a traveller coming from India is clearly at higher risk of carrying the virus than one from Rwanda. This should be reflected in an amended policy.
We propose that countries with low caseloads be moved to the amber category. In order to do this, we recommend the government set out clear thresholds indicating when and for what reasons a country is likely to move categories. For example, in the EU, for restrictions on non-essential travel to be lifted for a given country, the number of Covid-19 cases per 100,000 inhabitants must be 75 or lower over the past 14 days.[_] The UK government should create a robust, transparent system for determining how countries are categorised for travel based on case rates, vaccination uptake and the level of testing conducted, all of which are clearly communicated to the public.
Putting Travel Testing on a Long-Term Sustainable Footing
In the medium term, over the next 12 months, we believe the country should move to a more durable position. This is based on the UK being fully vaccinated, and only relying on boosters, during this time. Such a shift in approach would have to fit alongside global coordination on travel requirements and a Covid ID being used.
Critically, the strategy also seeks to put the testing regime on a sustainable footing by switching emphasis to lateral flow testing. While there is current PCR-testing headroom to work with, this is not likely to remain. Lateral flow testing, by contrast, can be scaled, is widely available and is cheaper.
The world is likely to be living with Covid-19 for the foreseeable future. Living and travelling safely in this context requires a robust, transparent, flexible and affordable travel system.
By 2022, we believe the government should take the following steps:
Embrace Lateral Flow Testing
Fully position lateral flow tests as the basis of the testing regime. We accept that, as a rule of thumb, PCR tests are considered more accurate, but the lateral flow alternatives are more useful for these specific things:
They detect those carrying the virus who are infectious.
They are cheap.
They produce very quick results.
They remove the need for lab infrastructure.
They can be scaled more easily.
With each aspect of the Covid-containment architecture, it is important to bear in mind that a calculus of risk is needed between safety, feasibility and economic viability. In the case of travel testing, we believe medium-term PCR testing as a default will prove less helpful because of turnaround times and the infrastructure it requires. Private testing providers are already reporting issues with turning tests around in time for travellers to go abroad. This will only grow as more people travel in the coming months and years. By contrast, moving to a position of lateral flow testing by default would remove the constraints on these turnaround times and costs.
The UK has already been on a significant journey of increasingly turning to lateral flow testing. It is now the workhorse test for population-level testing. Key figures in the scientific community have endorsed its value. Sir John Bell, Regius Professor of Medicine at the University of Oxford, said: “These inexpensive, easy to use tests can play a major role in our fight against Covid-19. They identify those who are likely to spread the disease and when used systematically in mass testing could reduce transmissions by 90 per cent.”
To ensure this testing is robust and capable of detecting new strains, we would suggest that positive tests be backed up by a confirmatory PCR test that can be sent for genomic sequencing. This PCR testing would be done via NHS infrastructure for free.
This shift in testing approach would be carefully monitored by the government to ensure sufficient number of positive cases are being detected and that new variants are being identified. This oversight would ensure PCR testing is drawn down and lateral flow testing dialled up in a sustainable and careful way.
Reduce Quarantine Requirements
In the context of a fully vaccinated population and regular testing, we believe the quarantine system can be refined and reduced.
Drop automatic quarantine for amber list countries.
Recommendations
To get the country fully moving again, with greater numbers of passengers travelling, the UK needs a robust, simple and cost-effective travel system of the kind we have set out.
Simplifying and making the current travel system viable requires a series of steps over the short and medium term. We set these out below as concrete recommendations.
Short term (2021):
Reduce the cost of testing by drawing on NHS PCR capacity and offering it at low cost.
Differentiate between vaccinated and unvaccinated travellers. Remove the need for vaccinated travellers to isolate when returning from an amber list country.
Medium term (2022):
Move to a position of routinely using lateral flow testing for travel testing.
PCR tests can then be used to verify positive lateral flow test results.
As all passengers become vaccinated, the need to quarantine when returning from amber list countries would be fully removed.
Chapter 6
Over 1.3 million new users signed up for the NHS App between 7 May (when the ability to show vaccination status was announced) and 23 May. The NHS App now allows users to log in securely, check their vaccine record and show proof of their vaccine status (type of vaccination, number of doses and date of vaccination). As this app is linked to NHS records, vaccine status will automatically be updated on it in the form of text and a 2D barcode (with an expiration date). The NHS App is different from the NHS Covid-19 app – which is part of the NHS Test and Trace service and is primarily used for contact tracing while providing information on local area restrictions, venue check-in and recording of PCR test results (which must be entered manually). At present, vaccination status and PCR test results are recorded separately on these two apps.
Globally, many countries and organisations are working on the concept of health passports to enable and facilitate seamless cross-border travel. Such seamless cross-border travel has been implemented in countries such as Bahrain, which launched a digital Covid-19 vaccine passport in Feb 2021. Bahrain’s BeAware app displays a green shield alongside an official certificate detailing the person’s name, date of birth, nationality and which vaccine was received. Users must have received two doses of a vaccine, separated by 21 days, and then wait for two weeks for antibodies to develop. Authorities can verify its validity by scanning a QR code that links to the national vaccine register. This can be used for travelling to countries like Saudi Arabia, which exempts the Bahraini certificate holder from PCR tests and quarantine. Similarly, arrivals to Saudi Arabia from countries like Hungary, Cyprus and Greece with mutual recognition of vaccination certificates will not be required to undergo PCR tests upon arrival, if evidence of a recognised vaccine is provided. However, there might be some limitations in terms of which vaccines are currently being recognised.
The EU Digital COVID Certificate, expected to be introduced in EU member states from 1 July, is aimed at facilitating safe and free movement of citizens in the EU. It will represent a digital proof that a person has either been vaccinated against Covid-19, received a negative test result, or recovered from the virus. In principle, certificate holders will be exempted from free-movement restrictions; however, this may be subject to change if there are new variants of concern in certain member states.
In the UK, the Covid-19 vaccine status service in the NHS App is in principle designed to allow users to show their proof of vaccination easily for the purposes of international travel. However, several further improvements are needed if the NHS App is to function as a health pass either for international or domestic use. This is because:
As set out above, it does not allow users to prove their test status.
There is no clear way for other organisations to use it to check health status (and, in fact, the app guidance currently advises that only border authorities should use it).
It is currently accepted as a form of proof of vaccination status only by a few countries. Travellers are still required to follow alternative rules (for example, testing and, in some cases, quarantine) in most countries.
To allow for greater ease of movement in a secure manner, it is vital to ensure the global interoperability of digital health passes. Initiatives such as the Good Health Pass Collaborative are doing critical work to develop internationally recognised standards to facilitate interoperability – and, ultimately, universal acceptance – of digital health passes. It is crucial for global leaders to take collective and urgent action on standards harmonisation so that international travel can resume safely.
Recommendations
The government should update the NHS App to include PCR and lateral flow test results in one place, along with vaccination status. This should ideally happen in a secure, automated manner (i.e. PCR test results should be sourced direct from testing centres. The technology also exists to upload home lateral flow test results directly into an app so that they cannot be deliberately or accidentally falsified).
It should make available a partner-verifier app to organisations that want to take up the option to restrict access only to those at a reduced risk of spreading Covid-19.
More detailed guidance should be made available to individuals and organisations, explaining operations and security measures to help build trust in the app.
The UK should use its G7 presidency to coordinate mutual recognition of health passes, lending its weight to the work of the Good Health Pass Collaborative.
Testing
A Covid Pass should allow for testing data to give equivalent freedoms to the fully vaccinated for 24 hours.
And those opting for testing over a Covid Pass need to be aware of the risks that is posed to them.
This is the exception, and not the rule, allowing people who can’t have the vaccine for medical reasons to participate economically and socially.
The differences in accessibility, costs and validity between PCR and lateral flow tests ought to be considered (for example, PCR tests can be recorded/validated on the NHS Covid-19 app, but lateral flow tests cannot).
Chapter 7
Our ultimate aim should be to get the virus under control to the point where we can remove all restrictions and have no need for a Covid Pass. This will require the UK to hit the herd immunity threshold – which some estimates put at around 66 per cent – and for vaccines to be rolling out globally, which at the current rate could take until 2023.
While we’re working to reach the herd immunity threshold, we must make sure restrictions are as proportionate as possible. There is no need to limit freedoms for people who we know pose a very low risk of transmitting the virus. Clear guidance for businesses and a functioning Covid Pass will be critical to this.
As exemplified by Israel, the use of a Covid Pass can serve as an alternative to a blanket lockdown. Given the damage caused to the economy as well as to people’s mental health and wellbeing by full lockdowns, we should ensure this is an absolute last resort. A Covid Pass will allow us to keep society open while still proactively balancing the risks associated with the virus.
To get to this point the following steps are required.
Overview of Recommendations
General
Take account of an individual’s vaccination status when determining what restrictions they should be subject to.
Domestic
For as long as any restrictions are necessary, permit businesses and other organisations the option of removing certain restrictions for those who are at a reduced risk of transmitting Covid-19 (either because they are fully vaccinated or have a negative test) – once the vaccines have been offered to all age groups.
If they take up this option, they should be allowed to operate with no restrictions on capacity, no observed social distancing and without any requirement to wear a face covering.
Travel
Simplify the existing travel and testing systems with amendments for short- and longer-term strategies.
Reduce the cost of testing by drawing on NHS capacity and offering it at low cost.
Differentiate between vaccinated and unvaccinated travellers by removing the need for vaccinated travellers to isolate when returning from an amber list country.
Move to a position of routinely using lateral flow testing for travel testing and then relying on PCR tests to verify positive lateral flow test results.
Proving Vaccine Status
Update the NHS App to include PCR and lateral flow test results in one place, along with vaccination status. This should ideally happen in a secure, automated manner.
Make available a partner-verifier app to organisations that want to take up the option to restrict access only to those at a reduced risk of spreading Covid-19.
Publish additional, detailed guidance for individuals and organisations, explaining operations and security measures to help build trust in the app.
Coordinate mutual recognition of health passes using the UK’s G7 presidency.
Lead Image: Getty Images
Charts created and designed by TBI unless otherwise credited.